What is Scoliosis and What Causes It?
how we can help
Scoliosis Overview
Scoliosis is an abnormal curvature in the spine, leading to asymmetry in the appearance of the trunk and shoulders. Its cause is not completely understood. Given the advances in medicine in general and spine treatment specifically, this fact often surprises loved ones of patients. The fact remains, scientists have yet to determine the cause of scoliosis. Experts believe a combination of factors plays a role in the development of the disease.
This condition is a spinal deformity. This medical term refers to abnormalities in the shape, alignment, or curvature of the spine. Spinal deformity can be the result of congenital factors, developmental issues, or degenerative conditions. When present in children, regular monitoring may be necessary to ensure that the spinal curvature does not progress. Braces can be effective in managing mild spinal deformity in adolescents by holding the spine in alignment. As always, early detection allows for timely intervention.
According to The National Institute of Health, “Scoliosis is a sideways curve of the spine. Everyone has normal curves in the spine, and when looked at from behind, the spine appears straight. However, children and teens with scoliosis have an abnormal S-shaped or C-shaped curve of the spine. The curve can happen on either side of the spine and in different places in the spine.
The NIH notes “scoliosis is estimated to affect 4.5% of the general population. In a nation of approximately 273 million people, this means that over 12 million cases of scoliosis exist, and almost 500 more are diagnosed each day – about 173,000 every year.”
While there is no definitive cause of scoliosis, wide-ranging research suggests that there is a predisposition for the disease based on families of scoliosis patients. The mother-to-daughter inheritance rate for scoliosis is 1 in 4 or 25%, father-to-daughter is 1 in 10 or 10%, mother-to-son is 1 in 10 or 10% and father-to-son is less than 1 in 20 or 5%.
Table of Contents
Other facts about scoliosis are:
- About 3% of the people on the planet have a scoliosis curve that measures greater than 10 degrees, although the vast majority do not progress and only require observation.
- Book bags, sports, sitting slouched or other bad posture do not cause scoliosis.
- The most common type of the disease usually occurs in children aged 11 and older.
- Girls are more likely than boys to have this type of scoliosis.
- You are more likely to have scoliosis if your parent, brother, or sister has it.
- The ops of shoulders are uneven in scoliosis patents.
- One shoulder blade (in the upper back) is more prominent or visible than the other.
- One hip appears higher than the other.
- One side of the rib cage is higher than the other when bending forward.
- Pain or difficulty with heart function or breathing are not typically present in patients with scoliosis, but may become an issue in adult patients with severe deformity.
- Scoliosis may be associated with back discomfort, however, is not associated with debilitating back pain or neurological issues unless some other problem is also present.
With treatment, observation, and follow-up with the doctor, most children and teens have normal, active lives.
Symptoms
Diagnosing
Treatments
What is Scoliosis
According to Texas Back Institute spine surgeon Dr. Belanger, “Scoliosis is a side-to-side curve deformity of the spine that is greater than ten degrees. Patients can develop misalignment of their spine which can tilt them side-to-side or pitch them forward.

“Often the mild curvatures are tolerated well, but sometimes the curves continue to worsen and pose risks of significant deformity,” Dr. Arakal said.

“This condition can also cause a loss of height, restriction of rib cage and breathing,” noted Dr. Isador Lieberman, internationally respected expert on scoliosis. “Compression of the internal organs such as the intestines, lungs and heart, mechanical back pain, muscular back pain, nerve irritation, spinal cord compression, unappealing physical appearance with rib hump, prominent hip, asymmetric shoulders are also possible.”
Patients Ask:
What is degenerative scoliosis?
Texas Back Institute Responds: Over time, a patient with this disease can experience degenerative scoliosis. This is also called “adult-onset scoliosis.” This condition describes a side-to-side curvature of the spine caused by degeneration of the facet joints and intervertebral discs which are the moving parts of the spine. This degeneration and resulting spinal asymmetry can occur slowly.

What Causes Scoliosis?
According to analysis from the NIH, In most cases, the cause of scoliosis is “idiopathic” which means it is unknown. Researchers continue to study possible causes for idiopathic scoliosis and adolescent idiopathic scoliosis. They think that a combination of several factors may lead to the disorder. These include:
- Genes.
- Hormones.
- Changes in cell structure.
For some children, scoliosis happens when another disease or disorder, or trauma causes the curving spine. These include:
- Congenital factors, which happen during the development of the spine when the baby is in the womb, leading to a curve in the spine.
- Genetic diseases, which happen when changes occur in one or more genes.
- Injury to the spine, usually from trauma to the spine or back.
- Neuromuscular diseases, which affect the nerves that send messages to muscles, leading to muscle weakness and loss.
- Spinal tumor, which can cause physical changes to the spine.
The spine specialists at Texas Back Institute note that scoliosis often occurs during the growth spurt just before puberty. While scoliosis can be caused by conditions such as cerebral palsy and muscular dystrophy, the cause of most scoliosis is unknown.
“The cause is multifactorial,” notes Dr. Lieberman. “Genetic predisposition, mechanical vulnerability, neurological contribution and asymmetric growth issues play roles.”
“Trauma might also play a role,” notes Dr. Arakal. “And it may be related to the physiology of the discs.”
Children who have mild scoliosis are monitored closely, usually with X-rays, to see if the curve is getting worse. In many cases, no treatment is necessary. Some children will need to wear a brace to stop the spinal curve from worsening. Others may need surgery to keep mild scoliosis from worsening and to straighten severe cases of scoliosis.
Is It Thoracic, Lumbar or Thoracolumbar Scoliosis?
The spinal condition of scoliosis can occur in three locations. With thoracic scoliosis, the curve is in the mid (thoracic) spine. Scoliosis in the thoracic area is the most common location for scoliosis to develop. Lumbar scoliosis has the curve located in the lower (lumbar) spine. As the name suggests, thoracolumbar scoliosis has vertebrae from both the thoracic and lumbar spinal sections involved in the curvature.
The spine specialists at Texas Back Institute note that most incidents of scoliosis in children are mild, but with age and growth, some curves can worsen. When this happens in the mid spine – thoracic area – the curve can reduce the amount of space within the chest and make it difficult for the lungs to function properly. This can cause breathing difficulties
Thoracolumbar scoliosis, when left untreated, can worsen over time. Gravity, everyday activities, and normal growth spurts can all contribute. Spine surgeons may recommend a brace if the curve is between 25 – 40 degrees. In any case, Texas Back Institute physicians will likely recommend physical therapy. Patients may be able to get injections to help manage pain. Healthcare professionals typically recommend surgery if the curve is more than 40 degrees or if your symptoms are severe.
Unfortunately, A scoliosis curve will not straighten on its own. Bracing will help to keep this spinal deformity from getting worse. Surgery in the form of a spinal fusion is the only procedure that will straighten the spine, and even this will not make it completely straight. Surgery will also stiffen the spine and is therefore reserved for more severe deformities.

Patients Ask:
Where is a spine surgeon who specializes in treatment for scoliosis near me?
Texas Back Institute Responds: There are several Texas Back Institute clinics throughout North Texas. Plus, many patients from around the world travel to the area to meet with the scoliosis specialists here. Click here to set an appointment and receive world class diagnosis and treatment for adolescent or adult scoliosis.
Diagnosing Scoliosis
As is the case with many childhood diseases, the “first line of defense” for scoliosis is often a school nurse. The nurse will usually use the “Adam’s Forward Bending Test,” which has the child bending forward at the waist and reaching his or her arms straight outward. Abnormalities such as a protruding rib or an abnormally shaped back may be seen. Scoliosis can also be diagnosed during routine pediatric exams.
The physician will examine the spine, hips, shoulders, and legs to assess for signs of scoliosis. If scoliosis is suspected, X-rays may be ordered to confirm the diagnosis and determine the severity of the spinal curvature. A child’s scoliosis is determined by the shape, size, direction, location, and angle of the curve.
Adult scoliosis is often diagnosed with X-rays taken during a search for the cause of back or leg pain. It may also be diagnosed when an X-ray is taken for an unrelated issue and the radiologist notices it on the X-ray.
Treatment for Scoliosis

The spine specialists at Texas Back Institute recognize and treat many different types of scoliosis, which are evaluated, and all are treated differently. These include:
- Idiopathic Scoliosis
This is most often in adolescence (age 10-17). It affects girls much more than boys and is passed down in families. There are also rarer forms that are present before age 10 and this form is not secondary to another condition.
- Neuromuscular Scoliosis
This refers to scoliosis that is secondary to some sort of neuromuscular condition or syndrome. Common ones would include cerebral palsy, myelodysplasia, muscular dystrophy, polio, spinal cord injury, and other conditions. These types of neuromuscular conditions cause muscles to become weak, spastic, or paralyzed. Without full support from the muscles of the back, the spine can develop an abnormal curve as it grows.
Signs of neuromuscular scoliosis often appear early in a child’s life. A parent or the child’s physician will most likely notice your child’s spinal curve through a change in their overall body position or when they start having trouble sitting in a chair. Symptoms may include:
- Leaning or uneven seating posture
- Using arms for seating support
- Uneven shoulder heights
- Head off center from the rest of the body
- Uneven hips or buttocks
- Uneven shoulder blades
- Arms hanging unevenly
- Degenerative Scoliosis
This is an adult-onset form that occurs secondary to the development of degeneration of the spine and its joints. This is most common after the age of 50.
- Congenital Scoliosis
Congenital Scoliosis is caused by abnormal development of vertebrae, present at birth. Sometimes vertebrae fail to form normally, or they can fail to segment from each other, leading to an abnormal curvature of the spine. This form can be noticeable at any age in childhood.
For children, treatment options for scoliosis are based on age, gender, and the location and severity of the curve. The curvature is monitored closely and, if necessary, managed with bracing.
While bracing is not a cure, it may impede the further progression of the curve. If the curve advances despite conservative measures or the measurement of the curve is greater than 40° to 50°, surgical correction is often considered.
With adult scoliosis, treatment planning is generally based on the severity of pain and functional limits. Because of the malalignment of the spine, pain may arise from the facet joints, sacroiliac joints, or from nerve root compression.
The pain from these conditions is managed with physical therapy, medication, facet injections, sacroiliac joint injections, or epidural steroid injections. If pain persists or physical function is significantly limited, surgery may be considered.
Posterior lumbar fusion (PLF), combined with pedicle screws and rods, is used to realign the spine. Sometimes, anterior lumbar interbody fusion (ALIF) is also done to create a 360° fusion – fusing the front and back portions of the spine.
Dr. Lieberman adds, “Patients diagnosed with this disease have several options for treatment. It’s important to maintain bone health and maintain physical fitness through exercise such as Pilates.
“We prescribe bracing for those who are in their growth spurt with certain types of progressive curves, medications for those degenerative curves with mechanical or neurological symptoms and as a last resort, surgery for those progressive curves in kids and for the progressive curves with debilitating pain and or neurological issues in adults,” he said.
Other treatment options include:
- Watchful waiting with serial observation of the curve
- Exercise & physical therapy
- Bracing
- Anti-inflammatory medications
- Surgery
Patients Ask:
Am I too old for scoliosis surgery
Texas Back Institute Responds: There are no age restrictions on scoliosis surgery. Age is only one factor that we will analyze to decide if surgery is reasonable to consider. Other factors include your other medical history, what surgery would be required, bone density, physical fitness, etc.
There are patients in their 80s who could have such surgery safely, and there are unhealthy patients in their 40s that we would not consider even a simple elective procedure because of the relative risk.
Halo-Gravity Traction for Scoliosis Treatment
In rare cases, spine surgeons at Texas Back prescribe a procedure called “halo-gravity traction.” This treatment is a method of gently stretching and straightening a severely compressed or curved spine.
Halo-gravity traction is often a first step in correcting severe scoliosis, kyphosis and other spinal deformities. Children remain in the hospital the entire time they are in traction, and this usually takes 3 – 8 weeks. After halo traction, children will usually have spinal fusion surgery to permanently stabilize the spine.
For children with severe spinal compression or severe scoliosis, halo traction reduces the risk of damaging the nerves or soft tissues that surround and support the spine during surgery. It is not considered a replacement for surgery, but it allows surgeons to begin to correct spine curvature with less invasive procedures.
In many ways, the halo-gravity traction is an ingenious method for helping prepare a child’s spine for the fusion procedure. Here’s how it works.
A surgeon will attach a lightweight metal ring (the “halo”) to the child’s skull with small pins. The pins go into the bone of the forehead to keep the child’s head from moving. Of course, the patient is given general anesthesia and is not awake for this procedure.
Once the halo is in place, a pulley system is activated. This system is attached to the child’s bed, wheelchair, and walker. Over the next few weeks, the physician will carefully add weight to the pulley to slowly straighten the child’s curved or compressed spine. Doctors use the child’s weight to decide how much weight to add.


What’s Involved with Scoliosis Surgery?
Surgical treatment for this disease has come a long way and it continues to evolve with better medical technology and surgeon training.
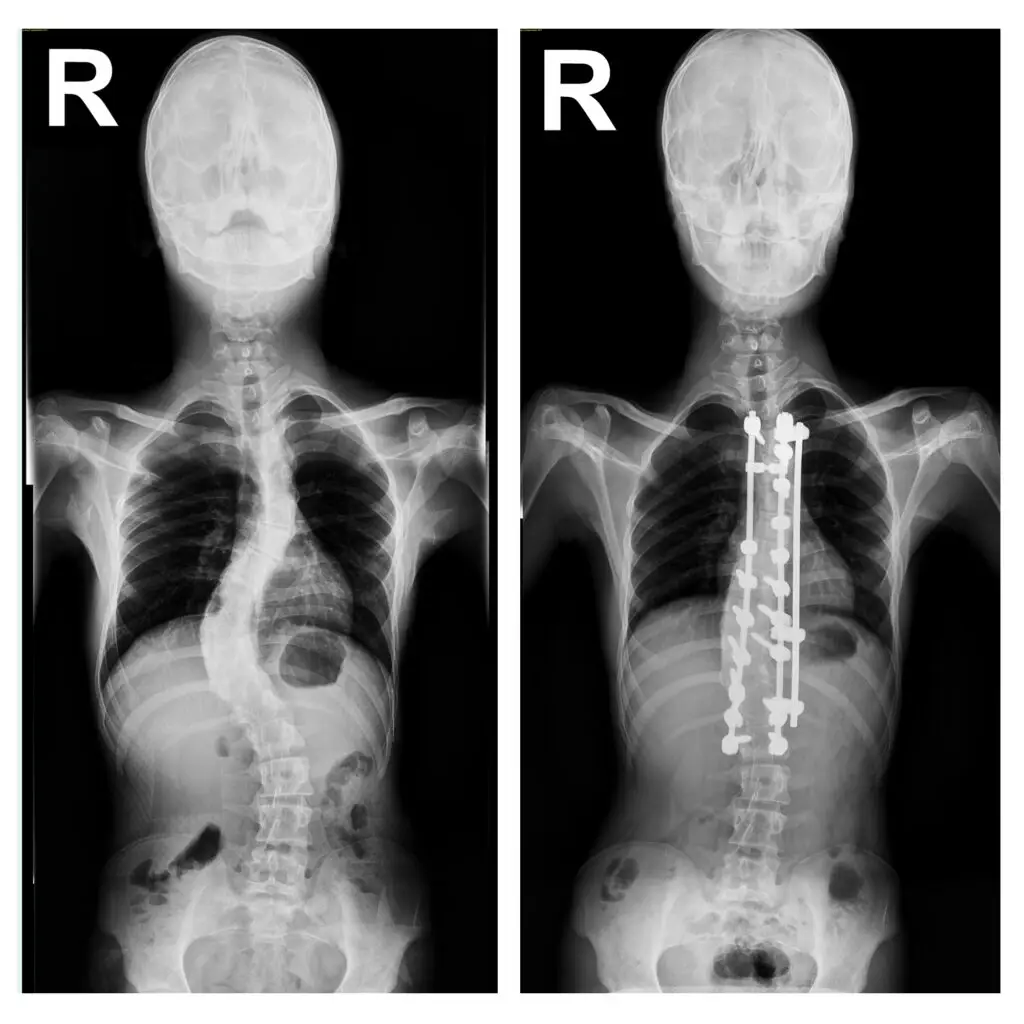
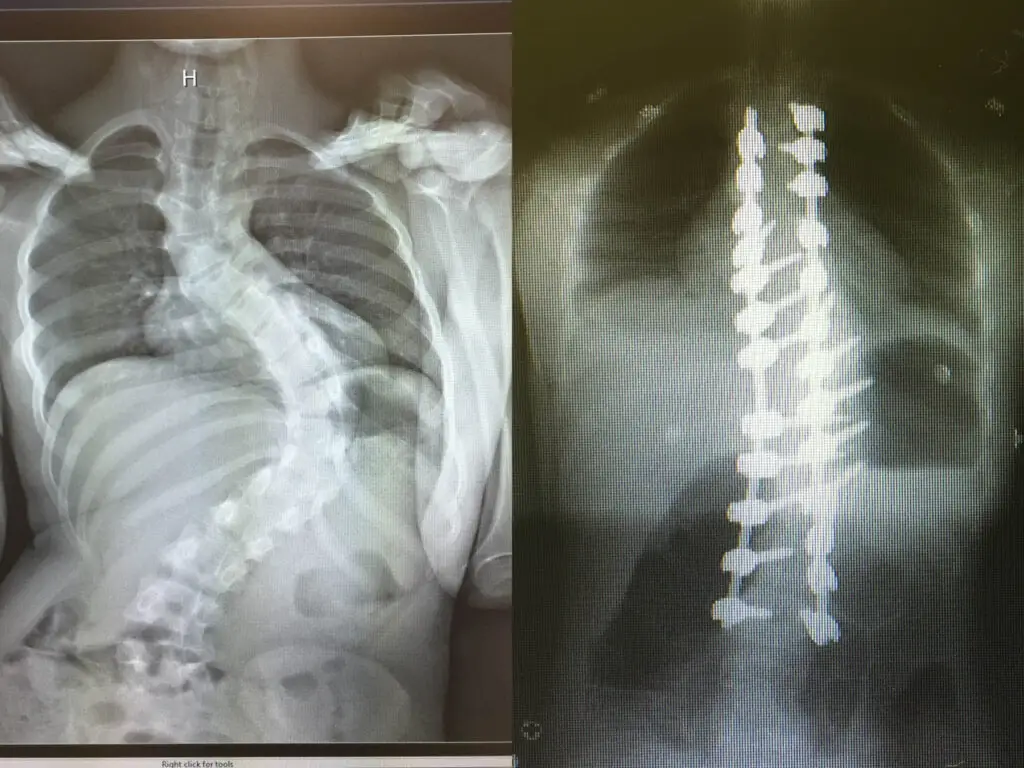
While surgery is always the last option used by the spine specialists at Texas Back Institute, with more challenging or deteriorating conditions such as neuromuscular scoliosis, stabilizing the spine with spinal fusion surgery (link to procedure or blog) is used. Using metal rods, hooks, screws, and wires, known as “instrumentation,” the procedure straightens the spine and solidifies the bone so it will no longer curve abnormally.
For six to 12 months after surgery, the spine fuses in much the same way that a broken bone heals. The child will need to wear a brace during this time. The instrumentation typically remains in the back without causing any problems.
The goal of a spinal fusion surgery for neuromuscular scoliosis is to:
- Stabilize the curve and stop its progression
- Balance the spine and pelvis (in patients who are unable to walk)
- Restore the ability to sit upright (in children who have lost this ability)
- Improve/preserve lung function
Spinal fusion for neuromuscular scoliosis is usually necessary by the time a child reaches adolescence — often sooner than with the milder idiopathic scoliosis. Compared to idiopathic scoliosis, it is usually necessary to fuse a larger portion of the spine to correct neuromuscular scoliosis.
The spine specialists at Texas Back Institute have extensive experience with surgery to correct conditions such as neuromuscular scoliosis. Because there is a potential for a higher rate of complications, safety is paramount throughout the surgical process – from preoperative planning through recovery. Texas Back employs a highly trained team of specialists, all working seamlessly, to mitigate any risk of complications.
What is Levoconvex Scoliosis?
When the curvature of the spine is to the left, this is known as levoconvex scoliosis. It is also referred to as thoracic levoscoliosis. This type of scoliosis affects the thoracic region of the spine, and it has an abnormal lateral curvature that goes to the left.
The spine experts at Texas Back Institute note with levoconvex scoliosis, there is an underlying pathology making the condition atypical. This could include neuromuscular conditions, a congenital malformation within the disc, trauma experienced by the spine, or tumors pressing on the spine, forcing it out of alignment.
Without treatment, levoconvex scoliosis can lead to serious health risks. Why? This is because the heart is located on the left side of the body. In severe cases, surgery may be required to address this curvature of the spine. However, treatment options such as physical therapy, exercises, and correcting poor posture help treat the condition. If it is left untreated, scoliosis can lead to issues such as injury and back pain.
If levoconvex is suspected, an examination by a spine surgeon should be considered.
King Richard III - Did He Suffer from Scoliosis?
Scoliosis has been referenced in medical literature for hundreds of years and has even been alluded to in a Shakespearean play – Richard III. However, when the Bard wrote the description of the king as “that foule hunch-back toade” he had no idea he was misdiagnosing Richard. New 3D visualization created by researchers and multimedia experts reveals that his scoliosis was the cause of his poor posture.
According to research published in the scientific journal “The Lancet,” King Richard’s poor posture and (and perhaps) his unpleasant demeanor seems to be the result of scoliosis. “We wanted to know if Shakespeare’s description was accurate, or an exaggeration to help legitimize the Tudor monarchs on the throne at the time,” study author Piers Mitchell, an anthropologist at the University of Cambridge said “Based on the study of his bones, Richard III would be better described as crook-backed than hunch-backed.
In a CBS News report aired in 2014, it was noted the royal skeleton was discovered under a parking lot in Leicester, England and DNA tests confirmed its identity five months later. To figure out the extent of the king’s scoliosis, the researchers created physical and computer-generated models of Richard III’s spine by performing CT scans and then using 3D prints of the bones based on the CT image data.
“The 3D visualization shows that Richard’s spine was curved to the right, and it was twisted to a degree, which gave it a “spiral” shape. The researchers also estimated that the king’s Cobb angle — a measure used to determine the extent of spinal deformities — was between 65 and 85 degrees — a curvature that would be considered significant these days. However, he also had a well-balanced curve, which means that his head and neck were straight and not angled to the side.”
“Richard did have a marked spinal deformity due to scoliosis,” Mitchell said. “However, there was no evidence from his skeleton for his having a withered arm or a limp, as portrayed in Shakespeare’s play.”
Richard’s scoliosis likely started to develop in the last few years of adolescent growth, after he turned 10, the researchers wrote in the study. The monarch’s right shoulder was likely positioned higher than the left one, and his torso was probably relatively short compared with his arms and legs.
The report also noted previous research has already shown that the king would have been about 5 feet 8 inches tall without his scoliosis. But the new study suggests that, because of his spinal condition, he may have appeared shorter than he really was. “This may have made him appear less imposing as a ruler,” Mitchell said.
Patients Ask:
What type of back brace is used for treating scoliosis?
Texas Back Institute Responds: There are two different types of braces for scoliosis: full-time and nighttime. Full-time braces are worn day and night, while nighttime braces are only worn while lying down. Some patients with scoliosis may only brace at night.
State-Of-The-Art Scoliosis Treatment
Any parent or spouse who learns that their loved one has scoliosis is shocked and saddened. There is nothing scarier than contemplating the ramifications of this diagnosis. However, with skilled surgeons and medical technology for treatment, and if necessary, fusion surgery, it can be managed, and patients can go on to have a productive, happy life.
The spine surgeons at Texas Back Institute are recognized throughout the world as scoliosis experts. They are waiting to help you. Please click here to set an appointment.
Learn more
Frequently Asked Questions
Over time, a patient with this disease can experience degenerative scoliosis. This is also called “adult-onset scoliosis.” This condition describes a side-to-side curvature of the spine caused by degeneration of the facet joints and intervertebral discs which are the moving parts of the spine. This degeneration and resulting spinal asymmetry can occur slowly.
There are several Texas Back Institute clinics throughout North Texas. Plus, many patients from around the world travel to the area to meet with the scoliosis specialists here.
Click here to set an appointment and receive world class diagnosis and treatment for adolescent or adult scoliosis.
There are no age restrictions on scoliosis surgery. Age is only one factor that we will analyze to decide if surgery is reasonable to consider. Other factors include your other medical history, what surgery would be required, bone density, physical fitness, etc.
There are patients in their 80s who could have such surgery safely, and there are unhealthy patients in their 40s that we would not consider even a simple elective procedure because of the relative risk.
There are two different types of braces for scoliosis: full-time and nighttime. Full-time braces are worn day and night, while nighttime braces are only worn while lying down. Some patients with scoliosis may only brace at night.
Locations